Patient guide
Embryo Genetic Testing in IVF: A Patient Timeline

Reticular Editorial Team
Patient Education

Embryo genetic testing can add a second wait to IVF. In the first one, you wait to see how embryos develop. In the second, after embryos are biopsied and frozen, you wait for the genetics report and the transfer plan. There are two waits because two different teams are doing the work.
That second wait can feel surprisingly non-linear. Retrieval does not always lead straight to transfer. A PGT cycle often includes embryo culture, biopsy, freezing, genetic analysis, results review, and a later frozen embryo transfer. At each stage, a different team is the one caring for your embryo.
That is the most useful way to read this timeline. Your embryo is handed from one team to the next, and the wait you feel is mostly the gap between those handoffs. Knowing who has your embryo at each step makes the quiet stretches easier to understand.
A gentle orientation
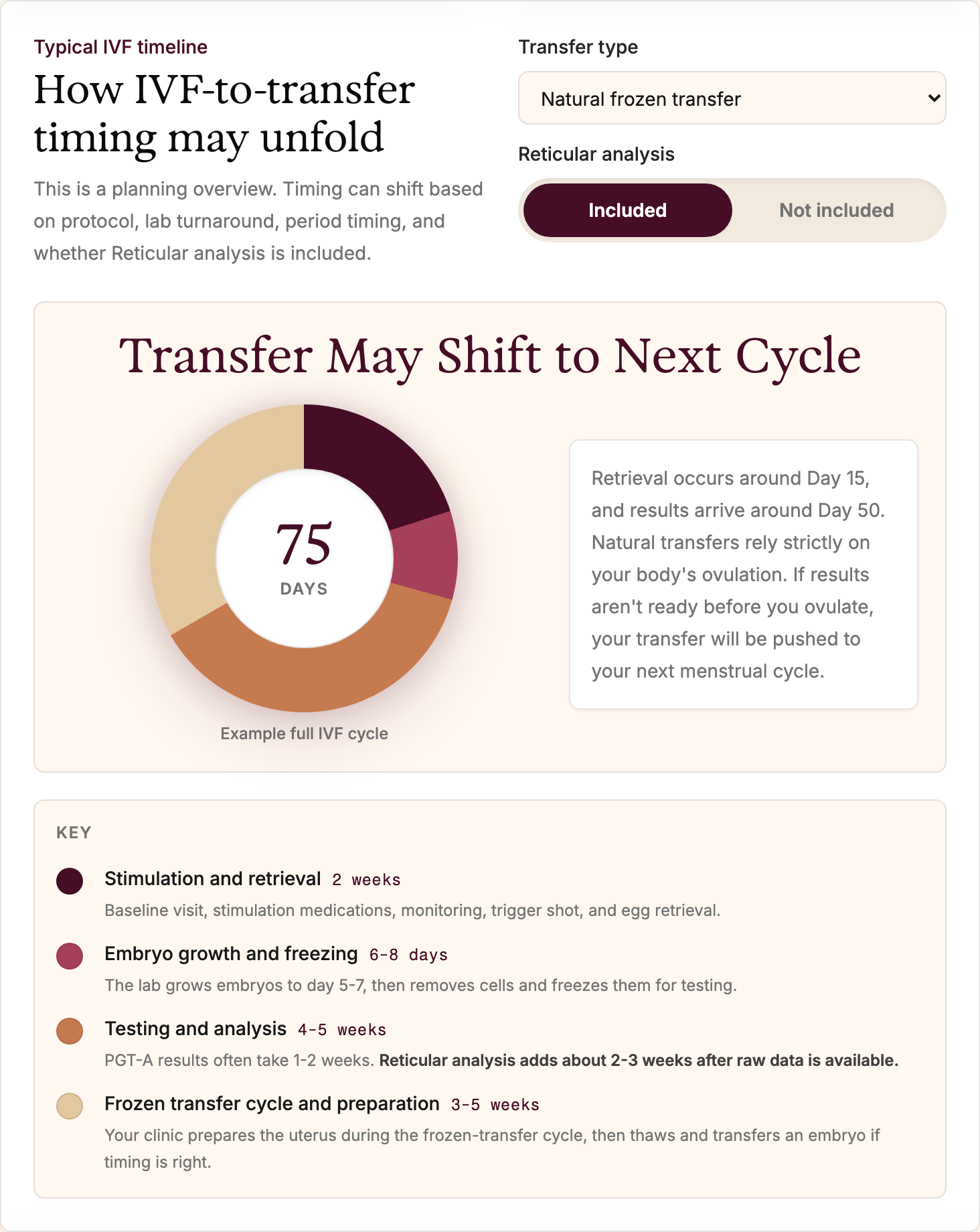
This is a map, not a fixed schedule. Your clinic's timing can vary by test type, lab, embryo development, result clarity, and whether the transfer cycle is natural or medicated.
Here is roughly how the pieces stack up in time. The exact days shift from clinic to clinic, but the overall shape — a stretch of stimulation, a short lab window, a longer testing window, and then a separate transfer cycle — stays fairly consistent.
Four teams are involved, in this order. The embryo starts and ends with your clinic, but in between it spends real time with the embryology lab and the genetics lab. Each phase below is labeled by whichever team has the embryo at that point.
1. Clinic
Medication plan, monitoring, retrieval, and transfer planning. Hands off to embryology after egg retrieval.
2. Embryology
Fertilization, embryo growth, grading, biopsy, and freezing. Hands the biopsy sample to the genetics lab.
3. Genetics lab
Sample analysis and report generation. Hands the results back to your care team.
4. Counseling and review
Result interpretation, counseling, and next-step decisions. Hands back to the clinic for transfer.
Before stimulation: deciding what to test for
The first decision is what you are testing for. PGT-A screens sampled embryo cells for chromosome number. PGT-M is used when there is a known single-gene condition or familial variant. PGT-SR is used for certain chromosome rearrangements.
SART's patient materials summarize these categories and emphasize that PGT decisions should be individualized based on age, medical history, preferences, and ovarian reserve (SART FAQ).
If PGT-M is part of the plan, the testing work may begin before medications start. ASRM describes PGT-M as technically complex because it can require genetic counseling, variant confirmation, case review, and laboratory test customization before an IVF cycle (ASRM PGT-M committee opinion). This is why some patients hear terms like "probe," "workup," or "case set-up."
Stimulation and retrieval
During ovarian stimulation, your clinic is still in charge: the team monitors follicle growth and hormone levels. When the timing looks appropriate, eggs are retrieved. At retrieval, the embryology lab takes over. It fertilizes the eggs and cares for any embryos that form.
Many labs use ICSI when PGT is planned, partly to reduce the chance of DNA contamination from extra sperm or surrounding cells. Your clinic can explain whether ICSI is recommended in your case and why.
This is also where attrition begins. Not every egg is mature. Not every mature egg fertilizes. Not every fertilized embryo reaches the blastocyst stage. Those drop-offs can be emotionally hard, and they do not mean you did something wrong.
A note about the numbers
IVF often feels like watching a funnel get narrower: eggs, mature eggs, fertilized eggs, blastocysts, biopsied embryos, embryos with reportable results. A smaller number at each step is common, even in well-run cycles.
Days 5 to 7: biopsy and freezing
This is the embryology lab's part of the process. Many current PGT workflows biopsy embryos at the blastocyst stage. ReproductiveFacts, an ASRM patient education site, describes PGT biopsy as taking a small number of cells from the outer trophectoderm layer around the fifth or sixth day after fertilization (ReproductiveFacts patient education). SART patient materials describe embryos often being frozen at the blastocyst stage, typically day 5 to 7 after fertilization (SART guide to ART).
Here is the key handoff: the biopsy sample leaves the embryology lab and travels to the genetics lab, while the embryo itself usually stays behind, frozen. If results will not be available quickly enough for a fresh transfer, freezing is what buys the genetics lab time to work. ESHRE's good practice recommendations note that testing platforms often require cryopreservation to allow time for genetic analysis, and that blastocysts should be cryopreserved promptly after biopsy when results will take several days (ESHRE biopsy recommendations).
Embryo growth
Some embryos reach blastocyst on day 5, others on day 6 or 7. Clinic policies for biopsy timing can differ.
Biopsy
The sample usually comes from trophectoderm cells, not the inner cell mass.
Freezing
Many PGT cycles use frozen embryo transfer so there is time to review results first.
Waiting for results
Now the genetics lab is running, and your embryo is frozen and safe while it does. This is usually the quietest part of the process, because the work is happening somewhere you cannot see. Turnaround time is lab-specific. PGT-A results may come back within days to a couple of weeks. PGT-M or PGT-SR can take longer, especially if the case is complex or needs additional review.
Before the report arrives, it helps to know the kinds of words that may appear:
- Euploid: the sampled cells appear to have the expected chromosome number.
- Aneuploid: the sampled cells appear to have missing or extra chromosome material.
- Mosaic: the sampled cells suggest a mix of chromosomally typical and atypical cells.
- No result or inconclusive: the lab could not produce a clear answer from the sample.
- Unaffected, affected, carrier, or at-risk: terms that may appear in PGT-M reports, depending on the condition and laboratory policy.
Results review and transfer planning
The report comes back, and your care team takes over again for counseling and interpretation, then the clinic handles the transfer itself. Results should be reviewed in context, not read alone. ASRM recommends that informed consent for PGT-A include risks, benefits, limitations, possible outcomes such as mosaic or no-result findings, and the option of not doing PGT-A (ASRM PGT-A committee opinion). For PGT-M, ASRM recommends genetic counseling before testing and notes that prenatal testing should be offered in pregnancies conceived after PGT-M because technical limitations can result in misdiagnosis.
After the review, your clinic may plan a frozen embryo transfer. Some patients move into the next available transfer cycle. Others pause for another retrieval, genetic counseling, uterine evaluation, finances, work schedules, grief, or simply a breath.
CDC's ART success-rate resources can help patients understand national and clinic-level outcomes, while noting that average success rates may not reflect an individual patient's chance of success (CDC ART success rates).
A checklist for each step
Here is a checklist to help you stay oriented at each step. Each item maps to a handoff, so you know what to ask of whichever team has your embryo at the time.
- Confirm whether you are doing PGT-A, PGT-M, PGT-SR, or a combination.
- Ask whether genetic counseling or lab customization needs to happen before stimulation.
- Ask which embryos are eligible for biopsy, including what happens with day 7 blastocysts.
- Ask whether embryos will be frozen after biopsy and when results are usually expected.
- Ask how mosaic, inconclusive, and no-result findings are handled before you receive them.
- Ask whether prenatal screening or diagnostic testing should still be discussed if pregnancy occurs.