Patient guide
How to Read an Embryo Risk Report

Reticular Team
Patient Education

Most embryo genetic reports answer one question: does this embryo have the expected number of chromosomes? A standard PGT-A report is essentially a list of embryos marked euploid (normal) or aneuploid (missing or extra chromosomes). That is genuinely useful — and it is also where most reports stop.

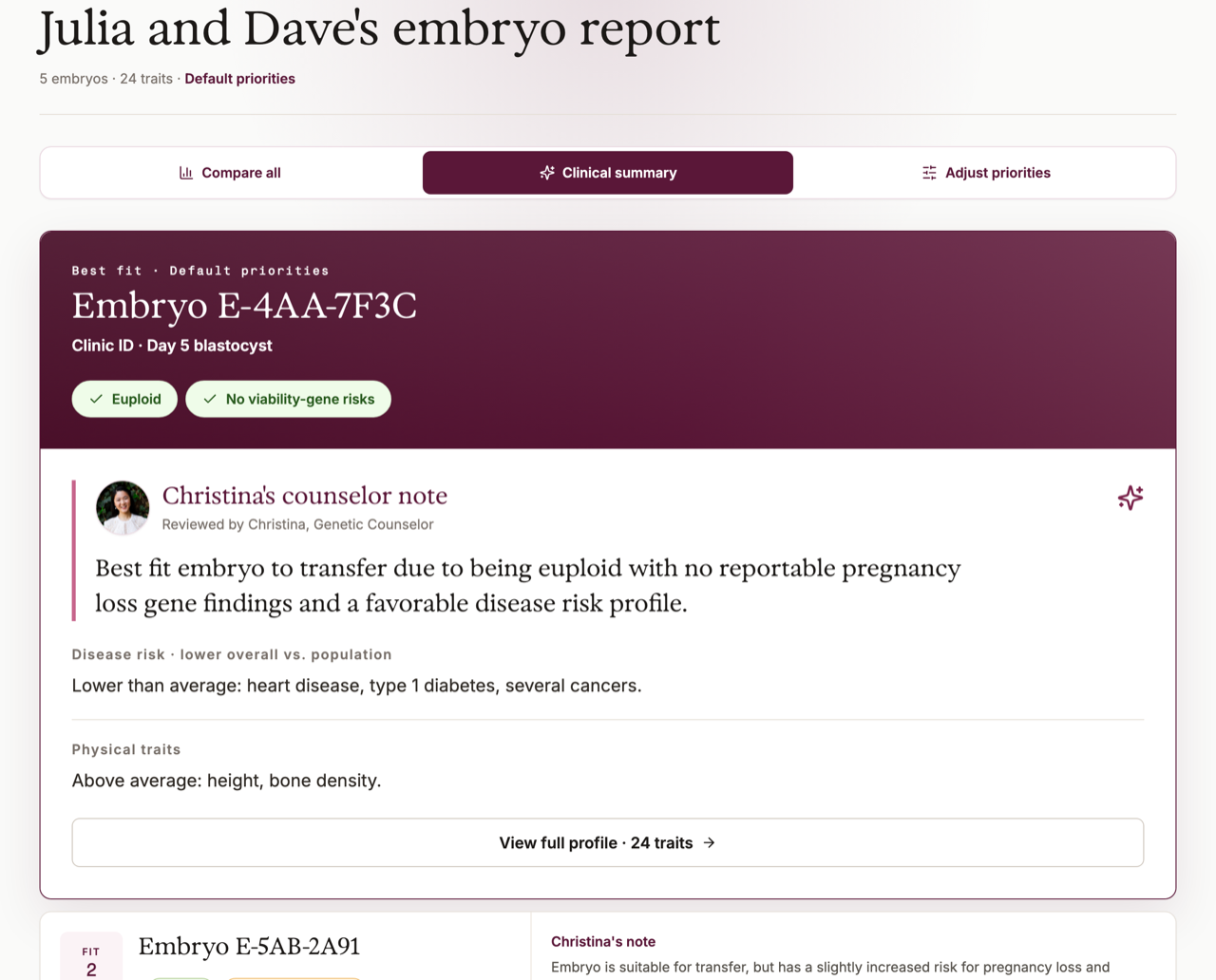
Some reports go further. Reticular's Embryo Complete report keeps that chromosome result and adds two more layers on top of it — a pregnancy-loss gene layer and a disease-risk and trait layer — and it opens with a plain-language note from a genetic counselor explaining what the report does and does not claim. Most PGT reports do not come with that note, which is exactly why a fuller report needs a way to be read. This walkthrough uses one as the example, but the order of weight it teaches applies to any report that goes beyond chromosomes.
A report like this is built in layers, and the layers are not equal. Read it from the most decisive layer to the least: first the chromosome count, then any pregnancy-loss gene findings, then the health-condition and trait estimates. Reading in that order keeps the softest, least certain part from driving a decision the firmest part should anchor. A risk estimate is not a diagnosis and not a transfer instruction, and every step here is something to bring to your fertility clinician and, when appropriate, a genetic counselor.
It is easy to do the opposite. The disease-risk and trait numbers feel the most specific, so the eye goes there first. But a polygenic estimate is the least settled thing on the page, and the chromosome result is the most settled. If you start with the soft layer, you can end up weighing a shaky number against a solid one as if they were equal. So go in order of weight, and point yourself to where each layer lives on the report.
If your report has a counselor note, start there
A standard PGT-A report will not include one. A fuller report like Reticular's opens with a plain-language note from a genetic counselor — and if yours has one, read it first. It tells you in sentences what the report looked at and what it is not claiming, and it is your map for everything below. The goal of the report is not certainty — every embryo, and every future child, carries some — and a good note says so plainly.
One more thing to know before the layers: "PGT" is not a single test. A reassuring result for one kind does not answer every genetic question, and the three layers below come from different kinds of testing with very different levels of proof behind them. Here is what each label means, so you can tell which layer a given section is built on:
PGT-A
Chromosome number
Looks for missing or extra chromosomes in the embryo sample. It does not screen for every inherited condition.
PGT-M
A known family variant
Looks for a specific single-gene condition or variant when the family already has a clear testing target.
PGT-SR
A chromosome rearrangement
Used when a genetic parent carries a structural chromosome rearrangement, such as a translocation.
PGT-P
Polygenic risk estimates
Uses many genetic markers to estimate relative likelihood for selected complex conditions. This is probabilistic and limited by the research data behind it.
Layer 1: Confirm the chromosome count first
The first and most decisive layer is the chromosome count. On the embryo summary card at the top of the sample report, find whether the embryo is euploid — the expected number of chromosomes — or whether the chromosome testing flagged something. This is the firmest result on the page, and it usually carries the most weight in whether an embryo is suitable for transfer at all. ACOG describes preimplantation genetic testing as testing embryos before transfer; the chromosome-count piece of that, PGT-A, is what this layer reports.
Read this result before anything else, because it sets the frame. A clear chromosome result does not screen for every inherited condition, but it answers the question your clinic usually weighs first. If the card shows a finding here, that is the thing to ask about before you spend any attention on the softer layers below — those estimates do not change what the chromosome count is telling you.
Layer 2: Look for any pregnancy-loss or viability gene findings
Next, look for any reportable single-gene findings tied to whether a pregnancy continues. These sit between the chromosome count and the disease-risk section in weight: they are specific gene findings, not broad estimates, and they speak to viability rather than to long-term health. On the sample report, this is where a named variant or a flagged single-gene result would appear with a counselor comment beside it.
Most reports will have nothing flagged here, and a clear section is good news worth reading plainly. If something is flagged, it deserves attention before the disease-risk numbers, because a finding tied to whether a pregnancy continues is more concrete than a polygenic estimate of adult disease. Read the counselor note attached to it, and bring it to your clinic as a specific question rather than letting it sit unexplained.
Layer 3: Read the disease-risk and traits last, and most cautiously
The last layer is the disease-risk summary and the traits section — the polygenic estimates and trait predictions. Read it last and read it most cautiously, because it is the softest and most uncertain part of the report. The ASRM Ethics Committee's 2026 opinion on PGT-P describes polygenic embryo screening as nascent and unproven, and says it is not recommended as a clinical service at this time. A polygenic line is not a clinical verdict, and it should not outweigh the two layers above it.
Because this layer is the easiest to misread, the rest of the steps below are about how to read it carefully. Work through them in order before you let any single number here shape how you feel about an embryo.
Read which condition the row is about, and how much genetics explains it
In the disease-risk summary, each row names a specific condition. Read the condition name first, before your eye jumps to its number — because the same word "risk" means very different things from one condition to the next. For a single-gene condition with a clear inheritance pattern, genetics explains a lot. For a common, multifactorial condition, genes are only one input among many.
So for each row, ask two things in this order: which condition is this, and how much of that condition does genetics actually explain? For a multifactorial condition, environment, screening, medication, age, and plain chance often matter as much as the inherited markers. A row that shows a number without telling you how much genetics explains is showing you only part of the picture. Knowing that much before you react to the value keeps a small genetic signal from feeling like a verdict.
Find the comparison group, then translate the number into people out of 100
Every value in the disease-risk summary is a comparison against something. A report usually compares the embryos already available in the same IVF cycle — not every possible future child, and not a settled yes-or-no about whether a child will develop a condition. Find what the number is being compared to before you react to it.
Then translate. Risk gets shown several ways, and some formats sound dramatic even when the practical difference is small. A twofold increase may sound large, but it could mean 2 in 100 instead of 1 in 100, or 20 in 100 instead of 10 in 100 — different conversations entirely. Whenever you can, convert what you see into people out of 100. Use this to turn each format on your report into the question that actually moves the decision:
| If the report shows... | Ask this next |
|---|---|
| A relative-risk label, such as "higher than average" | Higher than what baseline, and by how much in plain numbers? |
| A percentile or ranking | What absolute risk estimate does this correspond to, if known? |
| A small difference between embryos | Is the difference large enough to matter clinically? |
| A confidence range or uncertainty interval | How wide is it, and what assumptions are built into it? |
Check how much uncertainty the estimate carries
This is the step people skip most, and it matters most in this softest layer. On the sample report, look for anything that signals how confident the estimate is — a range, a confidence interval, an evidence-strength label, or a note about model limits. A single tidy number with no uncertainty shown is not more certain than a number with a wide range beside it; it just hides what the estimate does not know. So ask plainly: how wide is the range around this number?
This is also why ranking sibling embryos by these estimates is shakier than it looks. Sibling embryos can show different disease-risk numbers, but they share genetic parents, family history, and much of the same inherited background — so the differences are often smaller and less certain than a ranking implies. Before you treat one embryo as the "lower-risk" one, ask the report these:
Make the uncertainty visible
- How strong is the evidence for this condition?
- Which ancestry groups were well represented in the data?
- Was the model built from adult disease studies, embryo data, or both?
- How much do environment, screening, medication, and chance affect the condition?
- Has the lab changed model versions or reporting categories?
Kept in its place, this layer is useful context that sits beside the information your clinic already uses — not a replacement for it. Embryo grade, the chromosome result from Layer 1, age and reproductive history, uterine factors, medical considerations, and the clinic's transfer recommendations all still carry weight. Professional guidance leans the same way. ESHRE's PGT good practice recommendations discuss patient selection, counseling, pregnancy follow-up, and technical quality across PGT workflows. You should not have to make sense of a complicated report alone.
Remember what the report does not cover: pregnancy testing
After all three layers, one thing belongs in the conversation: embryo testing happens before transfer, while prenatal screening and diagnostic testing happen during pregnancy. They are not interchangeable, and none of the three layers above replaces them.
ACOG's prenatal testing guidance notes that preimplantation testing is not uniformly accurate, so prenatal screening and diagnostic testing should still be discussed with all patients. That does not strip the report of value. It means the report is one part of a longer care pathway, and reading it well should point you toward your next conversation with your care team, not close the topic.
Bring the report to your clinic with these in hand
You have now read the report in order of weight. These questions follow the same three layers, so you can point to the spot on your own report as you ask:
- What is the chromosome result for this embryo, and what does it mean for whether it is suitable to transfer?
- Are there any single-gene or pregnancy-loss findings flagged, and what do they mean for this embryo?
- For each condition in the disease-risk section, how much does genetics actually explain, and what baseline population was used?
- How wide is the uncertainty around these estimates, and are the differences between embryos large enough to change transfer planning?
- How does this report account for our family history, ancestry, and known genetic test results?
- Which parts of this are diagnostic, which are screening-level, and which are investigational?
- Would anything here change prenatal testing, pediatric follow-up, or health screening for either genetic parent?
One thing is worth watching for as you read this way. If, by the end, a single disease-risk number has become the whole decision — outweighing the chromosome result and any pregnancy-loss finding you read first — stop and ask your care team for a longer conversation. Reading in order of weight is what keeps the softest layer from carrying more than it can actually support.
If you already have PGT-A results
If your clinic handed you a chromosome-only PGT-A report and you want more from the same data, that is what Reticular's Embryo Complete report is built for. It re-analyzes your existing embryo sequencing — no new biopsy — and adds the pregnancy-loss gene layer and the disease-risk and trait layer on top of the chromosome result, with a counselor note to help you read it. The same order of weight still applies: the chromosome result anchors the decision, and the added layers are context to weigh, not a verdict.