Patient guide
The Limits of a Normal PGT-A Result

Reticular Team
Patient Education

When a normal, or "euploid," PGT-A result comes back, it is easy to read it as the genetic all-clear — proof that the embryo has been checked and nothing is wrong.
That reading is understandable, and it is not quite right. A normal PGT-A result is real, useful information. But it answers one narrow question, and it leaves several others completely open. This post walks through both sides plainly: what a normal result genuinely rules in, and what it does not rule out.
"Aneuploidy," the word behind the A in PGT-A, just means a missing or extra whole chromosome. So the test is asking one thing: does this embryo sample appear to have the expected number of chromosomes? Everything that follows comes back to that single question — and to the fact that it is only one question.
What a normal result rules in
For the question it asks, a normal PGT-A result is solid. The lab examined a sample from the embryo and did not detect a whole chromosome that was missing or present in an extra copy. That is the kind of difference behind conditions like Down syndrome (an extra chromosome 21), and it is the kind of difference most often linked to embryos that fail to implant or to miscarriage. Ruling it out, in the sample tested, is genuinely worth something.
ASRM's 2024 committee opinion describes PGT-A as focused on 24-chromosome copy number and notes that its value as routine screening for all IVF patients has not been demonstrated.
Rules in — for the cells sampled, within test limits
- A missing or extra whole chromosome was not detected (this is what "aneuploidy" means).
- The sample looked chromosomally typical across the standard set of chromosomes the lab reads.
- A common reason embryos fail to implant or end in early miscarriage — a whole-chromosome error — was not seen in what was tested.
Every line in that box carries the same two conditions: in the cells that were sampled, and within the limits of the test. These are not fine print — they are why the second list below matters.
Where even a normal result falls short
PGT-A is usually performed on a few cells biopsied from the trophectoderm — the outer layer of the embryo that is expected to form the placenta, not the baby itself. So the result is a reading from a small, peripheral sample, used as a stand-in for the whole embryo.
A few cells cannot show fine-grained detail. PGT-A is built to see whole missing or extra chromosomes, not small changes within a chromosome — a change far below that resolution can sit beneath what the test can detect. And embryos are not always uniform: when some cells read typical and others do not, the result may come back as mosaic. Reports can also land as segmental (part of a chromosome rather than the whole), inconclusive, or no-result. ASRM recommends counseling before testing about exactly these possibilities — no result, mosaicism, segmental aneuploidy, and the chance of misdiagnosis.
This is why the exact lab word matters. "Normal," "euploid," "no abnormalities detected," and "low-level mosaic" are not interchangeable, and if your report is not a clean euploid it is entirely reasonable to ask someone to read the actual wording with you.
Plain translation
The lab word is "normal." Read literally, it means: "in the few cells we sampled, we did not detect a missing or extra whole chromosome, as far as this test can see." That is narrower than "this embryo is genetically fine" — and it is the honest version.
What a normal result does not rule out
Here is the other side — the questions a normal PGT-A result simply never asked. None of these are failures of the test. They are conditions outside the one thing it checks, so a reassuring chromosome count says nothing about them either way.
Does not rule out
- Single-gene conditions in your family — a specific inherited variant, such as cystic fibrosis or a BRCA change, unless PGT-M was ordered for it.
- An unbalanced translocation — if a parent carries a chromosome rearrangement, that is the job of PGT-SR, not standard PGT-A.
- Sub-resolution changes — small additions, deletions, or new variants below what a whole-chromosome count can detect.
- Mosaicism the sample missed — cells elsewhere in the embryo that differ from the few that were biopsied.
- Common-disease risk — inherited risk for complex, many-gene conditions, which PGT-A does not estimate at all.
- Implantation and miscarriage — a euploid result improves the odds for some patients but does not guarantee a pregnancy or a live birth.
- The need for prenatal testing — screening or diagnostic testing in pregnancy is still its own separate step.
ACOG's preimplantation genetic testing guidance is direct about the bottom of that list: PGT cannot identify all fetal genetic abnormalities, and prenatal genetic screening or diagnostic testing should still be offered or discussed.
From pass/fail to a spectrum
Put the two sides side by side and the real shift becomes clear. A normal PGT-A result is a pass on one specific test — present or absent, expected count or not. It is binary by design, and for that one question that is exactly what you want.
But most of what shapes a future child's health does not live on a pass/fail switch. Risk for common, many-gene conditions sits on a spectrum, where two embryos that both passed PGT-A can still differ. The image below shows both at once — the pass/fail column on one side, the spread of risk on the other.
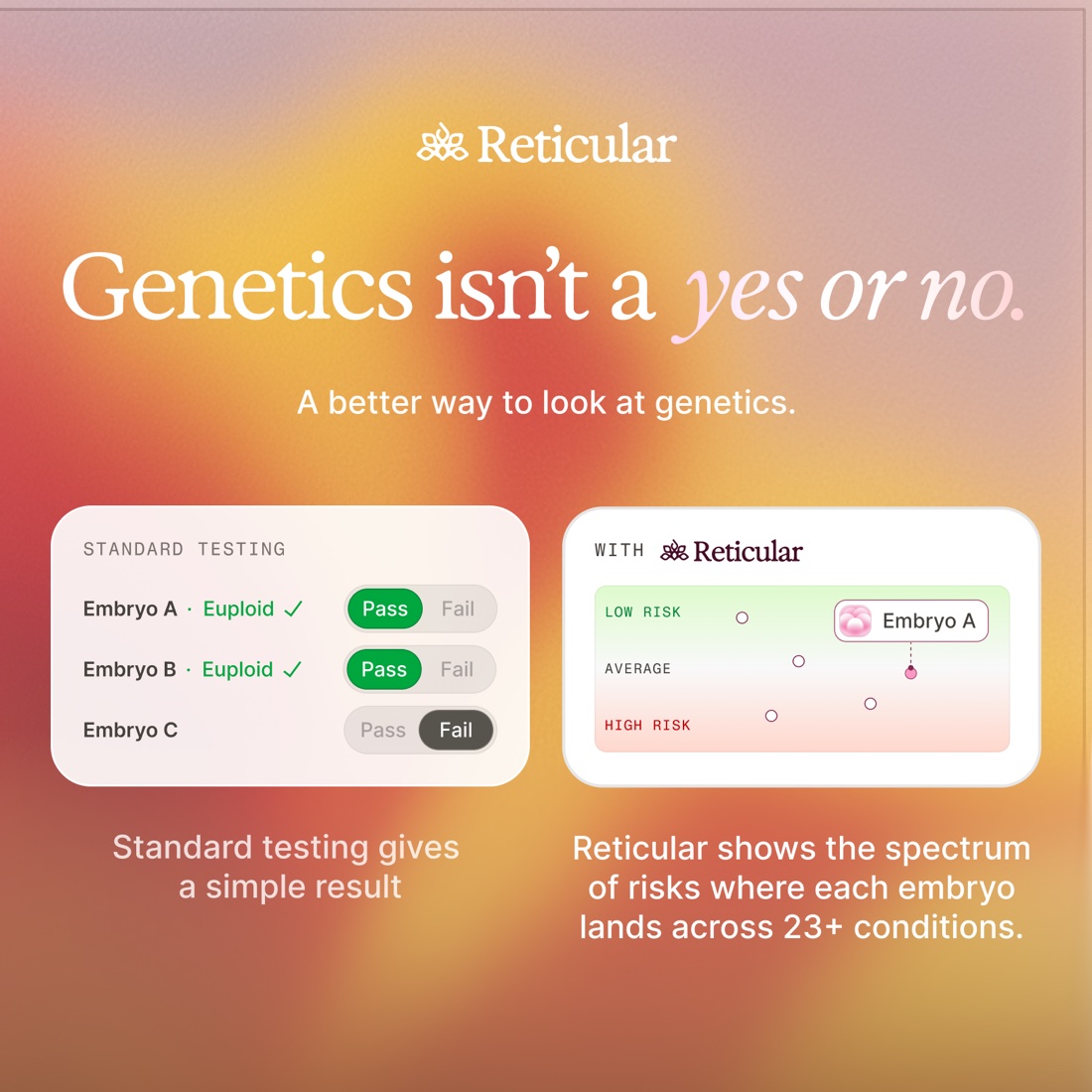
Reticular works on that second side. It does not re-check chromosomes or replace PGT-A; it estimates inherited risk for selected common complex conditions — context to weigh with the rest of your clinical picture, never a diagnosis or a transfer instruction. Two embryos with the same normal PGT-A result can land in different places on that spectrum.
PGT-A still earns its place in many IVF conversations, especially when chromosome-number risk is central — it can help a team decide which embryo to consider first when there is more than one. But the evidence is not the same for everyone: ASRM notes that recent multicenter randomized trials found similar overall pregnancy outcomes between PGT-A and conventional IVF groups in the populations studied, and that the effect on miscarriage reduction remains unclear. The sharpest question is rarely "is PGT-A good or bad?" — it is what problem is PGT-A solving in my case, and what is it leaving open?
So, plainly, here is what a normal PGT-A result actually tells you. In the few cells sampled from this embryo, and only as far as a whole-chromosome count can see, no missing or extra chromosome was detected. That lowers one specific risk. It says nothing, in either direction, about single-gene conditions, smaller or mosaic changes, family variants you did not test for, common-disease risk, or whether this pregnancy will take and stay — all of which remain open questions for your clinic and, when it helps, a genetic counselor.